
How Data Signals Shape Outcomes, Equity, and Economic Findings in Maternal Mental Health Research

Posted in Research Briefs What's New
Aditi Bhardwaj, MS; Wenjie Deng, MPP Candidate; Carol Davis, PhD, MBA
April 2026
Introduction
Perinatal mood and anxiety disorders (PMDs) affect a substantial share of pregnant and postpartum women, with documented consequences for maternal health, infant outcomes, and family well-being. Yet most U.S. retrospective health services research relies on administrative diagnosis codes ending up capturing only conditions formally diagnosed and billed (Luca et al., 2020).
In practice, screening and diagnosis are treated as interchangeable, creating a systematic blind spot: women who screen positive but are never formally diagnosed remain invisible to the datasets that inform funding and economic analysis. This gap falls disproportionately on younger, lower-income, and publicly insured women least likely to move from screening to diagnosis (Platt et al., 2024).
Using data from the Safe Babies Safe Moms (SBSM) initiative, we examine whether screening-based and diagnosis-based identification capture the same mothers and what is at stake when they don’t.
Data & Sample
Our sample includes 3,048 mothers who were screened for PMD — representing 42% of MWHC deliveries. Screening coverage within the broader 9,509-mother SBSM cohort increased over the study period: ~50% in 2020–2021 and ~53% in 2022.
We identified PMD using two independent strategies: (1) a positive EPDS or GAD-7 screen, or any affirmative self-harm response; and (2) mental health diagnosis codes in billing records (MMHC; captures mood and behavioral conditions, excluding substance use disorders). These strategies define four mutually exclusive groups: EPDS-only, diagnosis-only, both, and neither — enabling direct comparison of who each approach identifies and who it misses.
Key Definitions
This report uses the terms moms and mothers to refer to people who experience pregnancy and birth. We acknowledge that not everyone who gives birth identifies with these terms, and we aim to use language that is both inclusive and accessible.
Birthstay: The joint inpatient hospital admission for the mother’s delivery and the hospital stay of her newborn infant.
Screening: The standardized questionnaire used during prenatal care to identify symptoms of depression and anxiety (EPDS and GAD-7).
Diagnosis: A formal clinical determination documented in the patient’s billing records using ICD-10 codes. Maternal mental health conditions (MMHC) in this study are identified through behavioral major diagnostic code groups (mood and anxiety disorders) and obstetric-specific codes for postpartum anxiety and depression. Substance use disorder codes are not included. In this brief, MMHC refers to diagnosis-based identification.

Methods
Retrospective analysis using the full sample (n=3,048) for concordance and 958 PMD-signal mothers for PTB and economic comparisons. Screening was defined using MedStar thresholds (EPDS ≥10, GAD-7 ≥5, or any affirmative self-harm response). Diagnosis was defined by mental health diagnosis codes in billing records (captures mood and behavioral conditions, excluding substance use disorders).
Patients were classified into four mutually exclusive groups: EPDS-only, diagnosis-only, both, and neither. Chi-squared and Fisher’s exact tests compared patient characteristics. PTB rates and the differential in birthstay costs between full-term and preterm deliveries were tracked across 2020 and 2022 to assess trends as maternal mental health care bundles were implemented. The value of avoiding a preterm birth was defined as the difference in mean inpatient birthstay payments between preterm and full-term deliveries among PMD-identified mothers, estimated via Welch’s t-test (2022; 50% CI).
Results
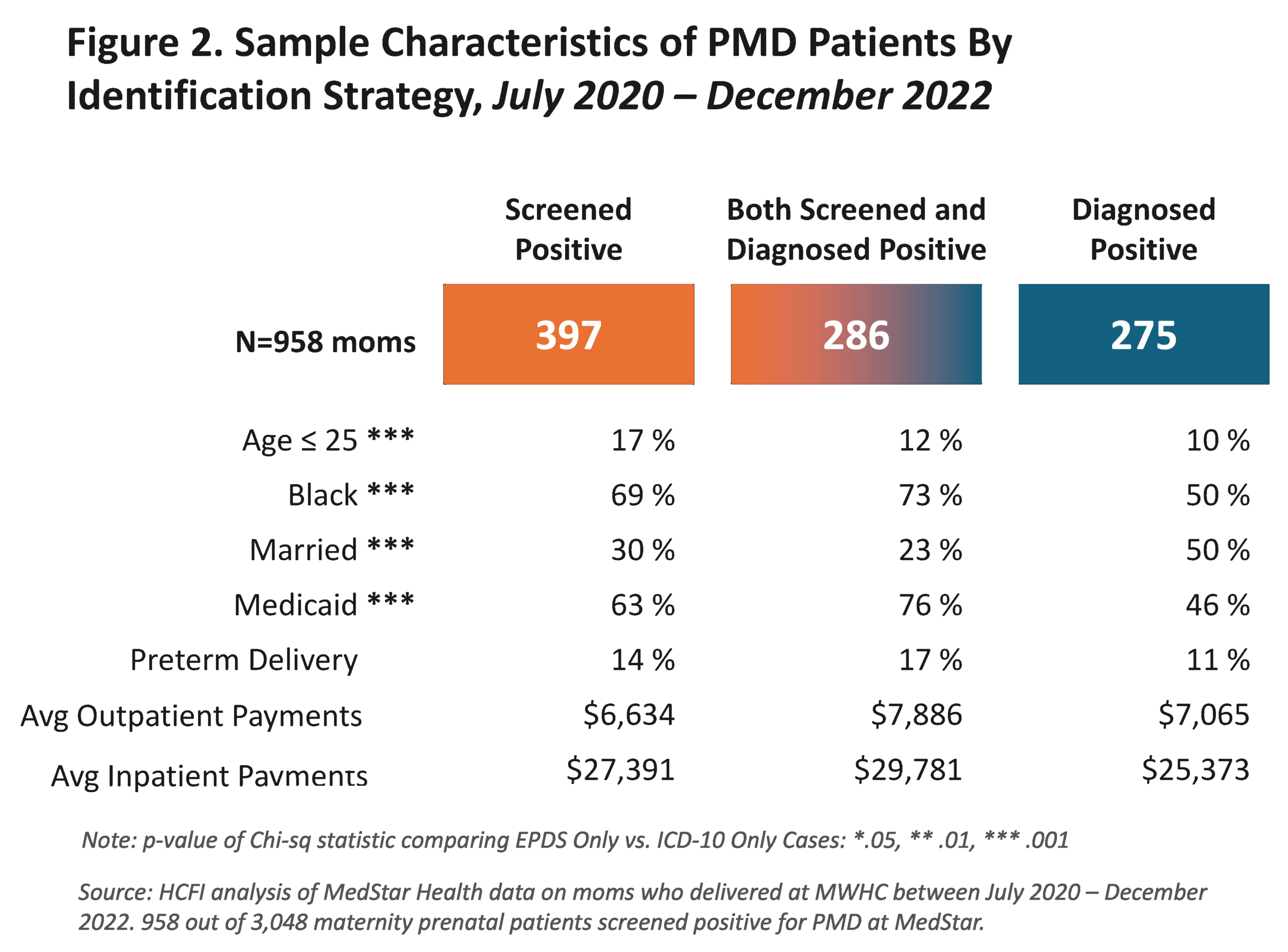
EPDS screening and ICD-10 diagnosis identification do not find the same mothers. Of the 3,048 mothers, 31% had at least one PMD signal — yet 13% were flagged by screening alone and 9% by diagnosis alone. Among the 958 with any PMD signal, the two groups differ significantly in race, age, marital status, and insurance — characteristics often associated with disparities — suggesting genuinely distinct populations, not the same women with different labels
ICD-10 missed 13% of EPDS-identified mothers — underrepresenting younger, Medicaid, and Black patients while masking real differences in preterm birth rates and costs of avoiding preterm birthstays.
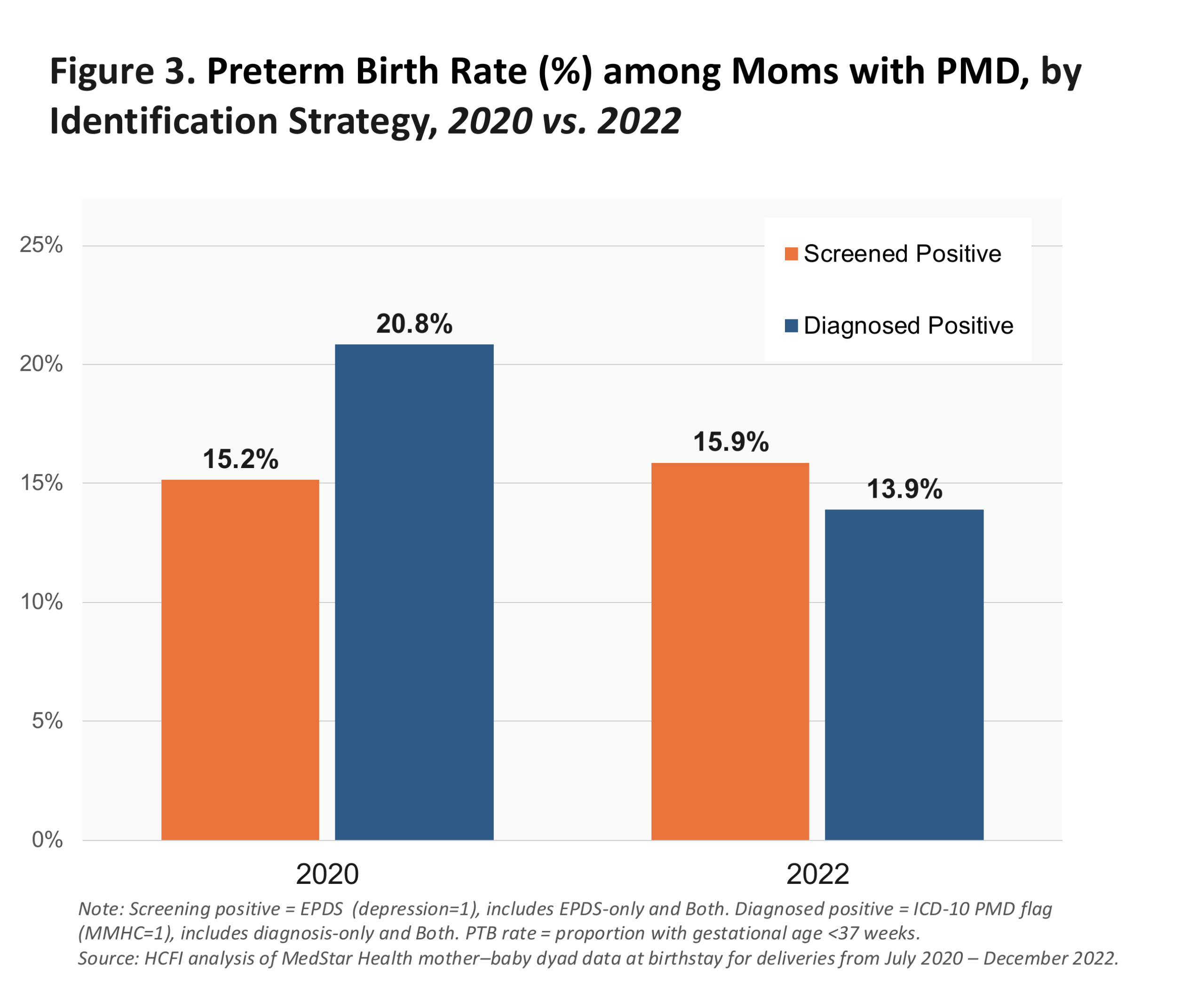
The two strategies also tell different stories about PTB trends (Figure 3). EPDS-flagged mothers showed a near-flat PTB rate: 15.2% in 2020 and 15.9% in 2022. MMHC-flagged mothers saw a sharp drop from 20.8% to 13.9%. The identification method determines whether you see stability or improvement.
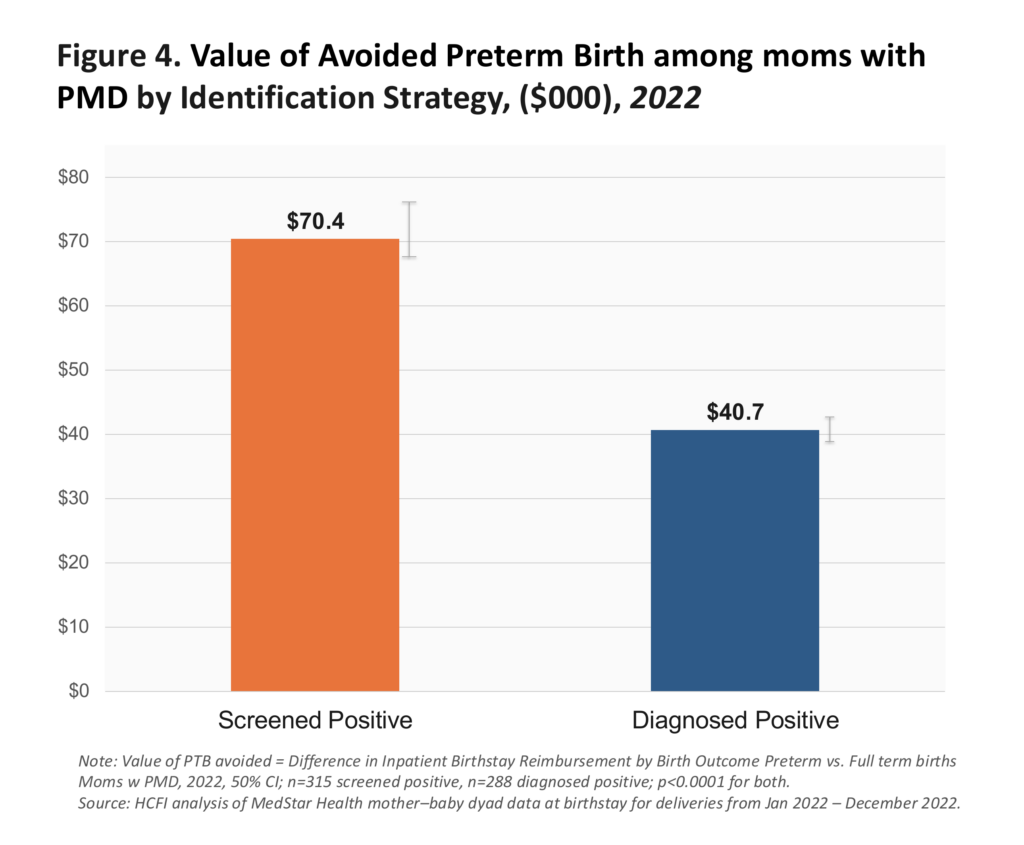
The economic picture shifts too (Figure 4). In 2022, the value of a preterm birth avoided was $70K among EPDS-flagged mothers versus $40K among MMHC-flagged — a 72% difference. Which population you identify changes the estimated economic case for the program.
Each of these three divergences — demographics, PTB trends, and economic value — arises from the same source: the identification strategy used. The lens shapes every downstream finding.
Conclusion and Implications
ICD-10 diagnosis alone missed 13% of sample mothers who screened positive on EPDS — underrepresenting younger, Medicaid-insured, and disproportionately Black patients while masking real differences in preterm birth rates and the economic value of avoiding preterm birthstays. As data scientists, we find that having both signals provides a more complete picture — making the case for universal EPDS screening not because it is clinically superior, but because it offers a standardized signal across a broader population. Paired with interoperable data infrastructure, this gives health systems and researchers the tools to make the strongest evidence case for programs like SBSM.
Limitations
• Findings are from a single hospital (MWHC, July 2020–December 2022). This limits
generalizability across settings and time periods.
• Screening practices evolved over the study period and not all eligible patients were
universally screened. Selection bias cannot be estimated or ruled out.
• PTB rates and economic burden estimates reported here are within-MedStar figures and
should not be interpreted as population-level projections.
References
• Patchen, L., et al. Safe Babies, Safe Moms: A Multifaceted, Trauma-Informed Care
Initiative. Maternal Child Health J 28, 31–37 (2024)
• Thomas, A. D., et al (2024). D.C. Safe Babies Safe Moms: A Novel, Multigenerational
Model to Reduce Maternal and Infant Health Disparities. NEJM Catalyst, 6(2), CAT.24.0161.
• Park, J., C. Dodd, J. Bhandari, and M. Munsell. 2024. “Impact of Mental Health Screening
Access on Incremental Cost Estimates among Patients with Postpartum Depression.”
Value in Health 27 (Suppl. 1): S107. Abstract EE273.
• Davis CB, Liaqat R, Bhardwaj A, Xu Y, Li V, DeLeire T. Toward Societal Return on
Investment from Safe Babies Safe Moms. Poster presented at MedStar Health –
Georgetown University Annual Research Symposium, (April 2024), Bethesda MD.
• Luca D. L., et al. (2020) Financial Toll of Untreated Perinatal Mood and Anxiety Disorders
Among 2017 Births in the United States. Am J Public Health. 110(6).
• Platt IS, Pendl-Robinson EL, Dehus E, et al. Societal costs of untreated perinatal mood
and anxiety disorders in Vermont. Arch Women’s Ment Health. 2024;27(4):585-594.
Acknowledgments
This work draws on data and evaluation questions developed during a project at MedStar Health Research Institute, funded by the A. James & Alice B. Clark Foundation. We thank Laurel Patchen, PhD, MSN, Vice-Chair, Obstetrics & Gynecology, MedStar Health Research Institute, and Aimee Danielson, PhD, Dir. Women’s Mental Health Program, MedStar Georgetown University Hospital for their insights on PMD identification strategies during the SBSM project.
Suggested Citation:
Bhardwaj A, Deng W, Davis CB. How Data Signals Shape Outcomes, Equity, and Economic Findings in Maternal Mental Health Research. Poster presented at MedStar Health – Georgetown University Research Symposium, April 2026, Bethesda, MD
About the Authors
All three authors are with the McCourt School of Public Policy at Georgetown University.
Aditi Bhardwaj, MS, Data Scientist, Massive Data Institute
Wenjie Deng, MPP Candidate, Graduate Student Research Assistant
Carol B. Davis, PhD, MBA, Assistant Research Professor & Associate Director, HCFI