
A Framework for Distinguishing Pediatric Primary Care Food As Medicine Programs Within the Food Assistance Ecosystem
Posted in Research Briefs SDOH What's New
Emmanuella Sobo, MPH, Saki Saito, Carol Davis, PhD, MBA
April 2026
Introduction
As health systems expand their role in addressing social determinants of health (SDOH), food insecurity has emerged as a priority need in pediatric primary care settings.1,2 At MedStar Health’s Department of Community Pediatrics (DCP), routine SDOH screening in 2025 found that 32% of patients screened positive for food insecurity and 11% identified needing assistance accessing public benefits such as WIC, SNAP, or Medicaid. DCP’s Food as Medicine (FAM) program is a program within the Center for Healthcare Innovation for Children and Families that provides food insecure patients access to seasonal produce markets, home delivered produce, and community resource navigation. While federal entitlement programs and community organizations form the backbone of food assistance, existing social care infrastructure was not designed to address the nutrition-sensitive health risks that present in clinical settings(1,3). This raises a practical question: when should scarce health care resources be used for food support if federal benefits and community groups already exist?
As part of an ongoing economic evaluation at MedStar DCP(4), we sought to articulate the conditions under which pediatric primary care adds incremental value and when referral to existing programs is the better course. Despite growing interest in SDOH integration, evidence frameworks for attributing health impact and guiding resource allocation remain limited(2,5), underscoring the need to define a clear and bounded role for clinical programs within the broader food assistance ecosystem(6,7).
Methods
We developed a 12-criterion assessment framework through a structured review of literature spanning health care management, performance management, and health services research and health economics. The framework is organized across two primary domains- Reach and Health Impact. We then applied the framework to profile four exemplar food assistance providers in Washington, DC: MedStar Health’s DCP FAM program, the Supplemental Nutrition Assistance Program (SNAP), the Capital Area Food Bank (CAFB), and Martha’s Table, using publicly available documents, IRS Form 990 filings, and stakeholder input. Three health economics team members independently scored each organization across the 12 criteria; results were synthesized into a Reach–Impact matrix and used to develop recommendations for program design, evaluation, and partnership development.
Results
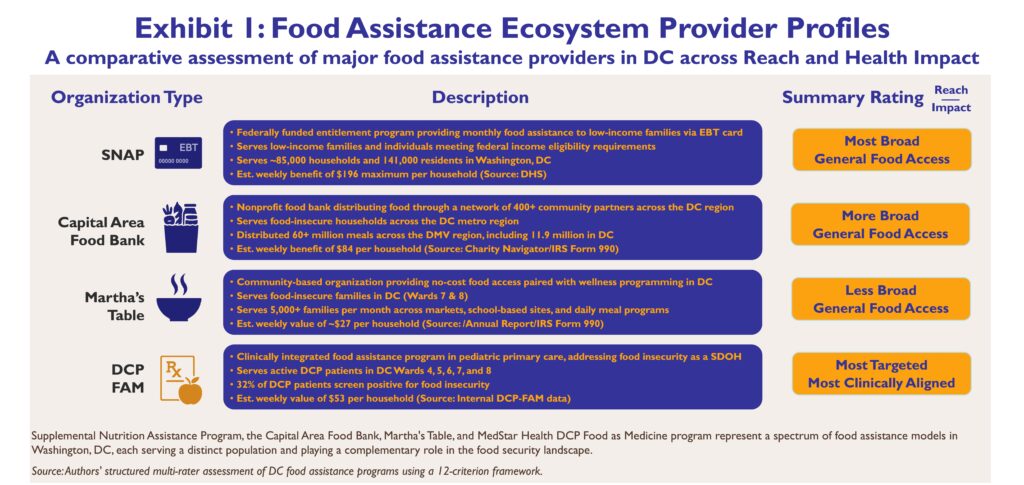
Exhibit 1 profiles four programs spanning the range of food assistance models in Washington, DC, illustrating how each differs in structure, eligibility, scale, and estimated weekly value delivered to households. Relative positioning was stable across raters, supporting the reliability of the 12-criterion framework as a consistent basis for comparison. As shown in Exhibit 2, federal entitlement programs like SNAP demonstrate the broadest reach, reflecting large enrollment capacity, stable federal funding structures, and a maximum weekly benefit of
$196 per household in Washington, DC. Community organizations occupy a middle position in the ecosystem, extending food access to residents seeking episodic assistance without strict eligibility requirements; CAFB delivers an estimated $84 per household per week across its network, while Martha’s Table provides an estimated $27 per household per week. The DCP-FAM program operates on a smaller, more controlled scale by design, as eligibility is limited to patients of the Department of Community Pediatrics and program capacity is shaped by available clinical staff and resources; the estimated weekly value of food provided is $53 per household. Within this defined population, DCP-FAM is best equipped to monitor and address nutrition-sensitive health risks, placing it in the clinically aligned, targeted quadrant of the Reach-Impact matrix. DCP-FAM is the only program among the four that screens for food insecurity as part of a clinical encounter and tailors its response to a child’s specific health needs. This highlights that pediatric primary care holds a distinct position in the food assistance ecosystem defined by its ability to assess imminent health risks and identify critical time periods where food insecurity can have the greatest impact on a child’s development and health trajectory. Taken together, all four programs occupy well-defined and complementary positions, each defined by the population it targets, the scale at which it operates, and the degree to which its services are clinically integrated.
Implications for Policy & Practice
…pediatric primary care holds a distinct role…to identify and respond to food insecurity in the context of nutrition-sensitive health conditions among the children it serves.
This framework demonstrates that pediatric primary care holds a distinct role within the food security landscape, not by replacing federal entitlements or community organizations, but by leveraging its clinical infrastructure to identify and respond to food insecurity in the context of nutrition-sensitive health conditions among the children it serves. Role clarity of this kind enables DCP and other clinical providers to connect families to the most appropriate resources while reserving clinical engagement for children with the greatest nutrition-related need. Sustaining this work requires demonstrating strong clinical outcomes linked directly to services provided — evidence that population-level programs like SNAP and CAFB are not structured to generate — and in doing so, strengthens the business case for long-term investment from Medicaid, health systems, and community sponsors.
Next steps include socializing the framework and community player assessments across the broader SDOH project team, including its implementation and community-based research arms, to inform future program design and evaluation, and to encourage similar frameworks tailored to the unique populations and food assistance landscapes of other communities.
Refernces
- National Academies of Sciences, Engineering, and Medicine. Integrating social care into the delivery of health care: moving upstream to improve the nation’s health. National Academies Press; 2019.
- Rangachari P, Thapa A. Impact of hospital and health system initiatives to address social determinants of health (SDOH) in the United States: a scoping review of the peer-reviewed literature. BMC Health Serv Res. 2025;25(1):342.
- Butler SM. Cross-sector support for a policy framework to tackle social determinants of health. JAMA Health Forum. 2024;5(11):e244809.
- Davis CB, Carrasco Hernandez E, Sobo E. Stewardship & sustainability: economic evaluation plan for pediatric food security interventions. Poster presented at: MedStar Health–Georgetown University Research Symposium; 2025; Bethesda, MD.
- Fichtenberg CM, Alley DE, Mistry KB. Improving social needs intervention research: key questions for advancing the field. Am J Prev Med. 2019;57(6 Suppl 1):S47-S54.
- Hinton E, Diana A. Medicaid authorities and options to address social determinants of health. KFF. Published January 29, 2024. Accessed April 13, 2026.
- Nikpay S, Zhang Z, Karaca-Mandic P. Return on investments in social determinants of health interventions: what is the evidence? Health Aff Sch. 2024;2(9):qxae114.
Acknowledgements
Our work is part of the Social Determinants of Health Innovation and Resilience Research Project and includes contributions from Georgetown’s Undergraduate CALL Internship. We acknowledge the leadership of Dr. Janine Rethy, MD, MPH, and the contributions of Joanne Odom, LICSW, and Shelby Wyand, MS, alongside partners from MedStar DCP, MedStar Center for Health Equity Research, the Health Justice Alliance (GU Law), and the Health Care Financing Initiative (GU-McCourt). This project was funded in part by the J. Willard and Alice S. Marriott Foundation.


Suggested Citation:
Sobo, E., Saito, S., & Davis, C. B. (April 2026). Distinguishing the role of pediatric primary care food as medicine programs within the food assistance ecosystem: A framework of reach and health impact [Poster presentation]. MedStar Health–Georgetown University Research & Education Symposium, Bethesda, MD.
About the Authors:
All three authors are affiliated with the Health Care Financing Initiative Research Center at the McCourt School of Public Policy at Georgetown University. Research at the Health Care Financing Initiative is focused on the economics, financing, and public policy of healthcare delivery in the U.S.
Emmanuella Sobo, MPH – Research Program Manager
Saki Saito – Undergraduate Student Researcher, CALL Intern
Carol B. Davis, PhD, MBA – Assistant Research Professor & Associate Director